


Sonic Healthcare performs more than 2,000 types of laboratory tests in our network, providing laboratory testing for about 100 million people globally each year. We thus have access to a massive amount of data that provides us with a unique opportunity to improve patient outcomes and generate value for healthcare systems. This article presents one example of how we worked with insurers and providers to bolster chronic disease care in the United States.
Data-driven population health management
In 2013, we collaborated with an insurance plan in California to identify specific patient cohorts that are imposing high costs on healthcare systems. By looking at the healthcare spending of 75,000 patients, we found that 88% of people spent only $314 per year and 11% spent roughly $5,000 per person per year. The remaining 1% spent $61,000 per year on average, a relatively huge amount. Many of these people had chronic kidney disease (CKD), diabetes and other common chronic diseases that account for a disproportionately high share of healthcare costs.
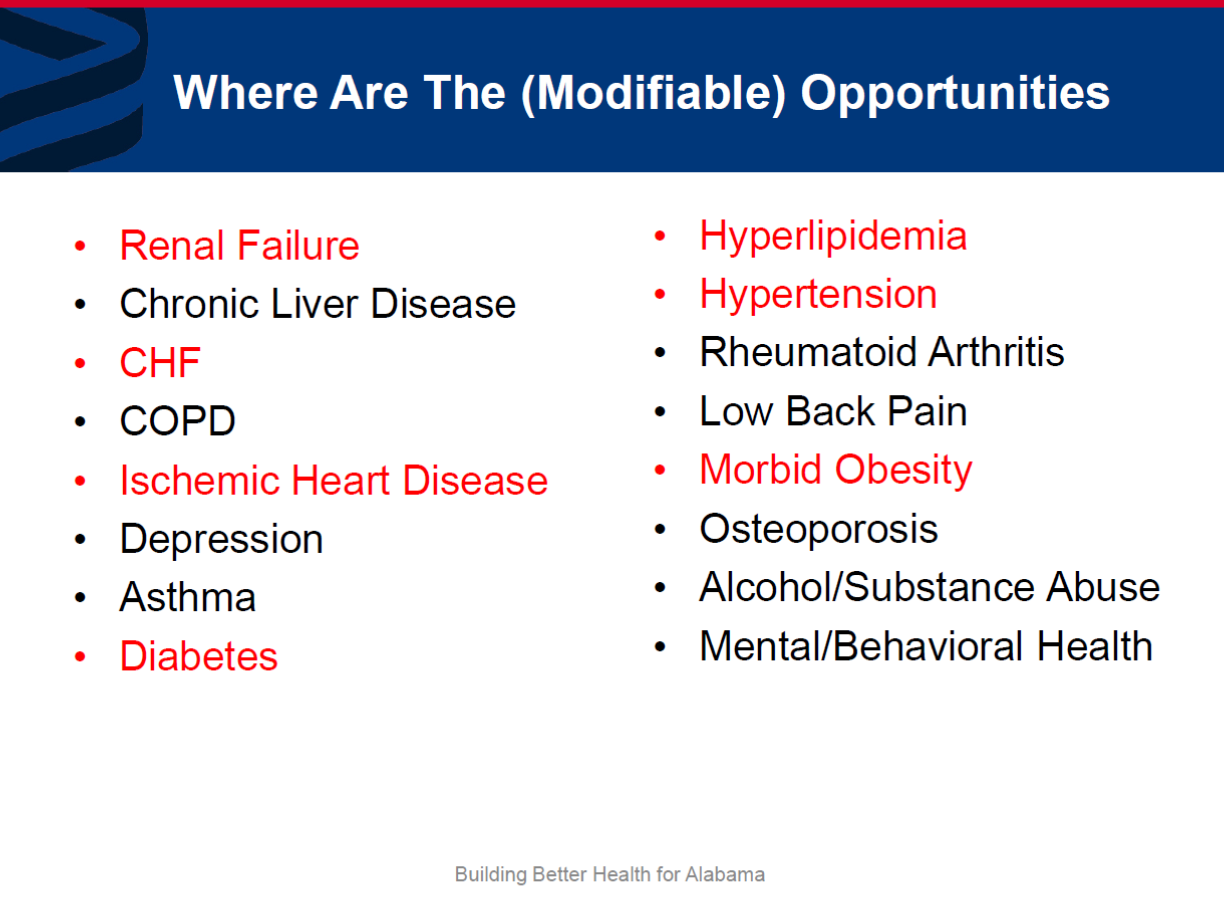
We followed this high-spending group and found that only 38% of these patients stayed in same bracket for two years in a row. All the others were in a lower-spending bracket the previous year. For many, this jump was due to cost of treatment and complications from 16 chronic conditions with particularly high costs per capita (see image below – conditions in red are common comorbidities).
Identifying gaps in diabetes care
Focusing on type II diabetes, we found that many patients often failed to make follow-up appointments after receiving a diagnosis, leading to costly complications. Examining HbA1C laboratory data at a large primary care practice caring for 50,000 patients, we identified nearly 3,800 diabetic patients who met diagnostic criteria, but found that 26.5% of them had not seen their doctor in the past 12 months and 700 did not have an associated ICD diagnosis code.
Among the patients that did receive a diagnosis, we expect that some were asymptomatic and did not fully understand what conditions they were being tested for, and never returned see their doctor because they didn’t feel sick. These laboratory results would then sit in the patient’s chart, with no action being taken until the disease progresses to a point when a sudden exacerbation of their condition resulted in an emergency room visit and an expensive admission – hence the spending spike from one year to the next.
Next, we partnered with a large practice in New York that was involved in the care of approximately 80,000 patients. Applying our analysis, we identified 1,200 patients overdue for a follow-up appointment. A patient list of this size posed considerable challenges. Firstly, manually contacting everyone would have been impossible, and secondly, the sheer volume of patients required a system to triage whose cases were the most urgent.
In the absence of necessary manpower, innovation was key. We developed a new mobile technology that sends automated emails, calls, text messages or a template letter to alert a patient that they are overdue for follow up. We then used our lab data to determine which patients were at the highest risk of health exacerbations within the next six to 12 months. These were the individuals for whom contact was prioritised.
A particularly successful element was that the doctor’s own voice was pre-recorded to make these automatic calls. During the call, the patients would be told that they had doctor-ordered laboratory tests to complete before their consultation. When the patient came to clinic, the lab results were already available, and the doctor could review the results and treat the patient accordingly.
The process was simple for doctors too—each week, they received a list of patients overdue for visit. In three clicks, they could confirm the patient list, reauthorise the ICD diagnosis codes or add new ones, and authorise orders for laboratory testing.
Proactive interventions for clinical improvements
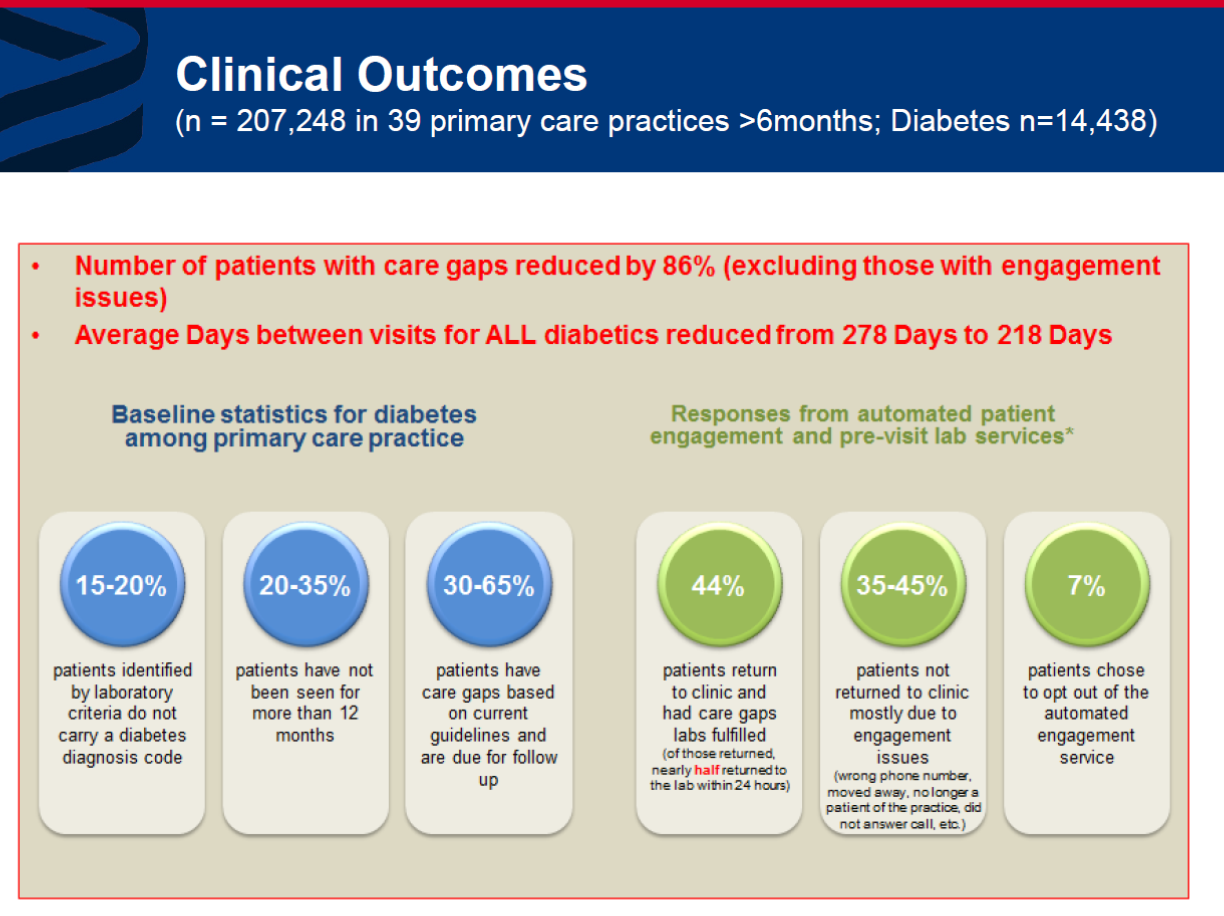
This process began 3.5 years ago, and we have since partnered with 39 primary care clinics covering more than 200,000 patients. The results were surprisingly positive—44% of the people we contacted for follow-up returned to see their doctors, and only 7% opted out of communications. We saw an 86% reduction in the number of patients with gaps in care, and a significant increase in the frequency of doctor visits.
An earlier NIH-funded study into a similar follow-up system tracked patients for 5 years and found a saving of US$2,400 per person per year to the healthcare system, as well as reduced hospital stay and reduced emergency room visits. The results from this study and our data both show that keeping patients engaged in their own healthcare and facilitating early interventions is worth the initial investment of resources. Following the success of the diabetes follow-up program, we have since expanded into CKD and 6 additional conditions.
By using lab data proactively and developing innovative solutions to address gaps in care, our experience shows that laboratories can drive improvements in the healthcare sector for both physicians and patients alike.
This article is based on the presentation “Integrating pathology data analytics and patient engagement is a value- and outcome-based care delivery” at the Roche Efficiency Days (RED) 2018 REDefining perspective in Guangzhou, China.





