





Rapid and safe diagnosis of acute myocardial infarction (AMI) is of major medical and economic importance because it facilitates the timely treatment of chest pain and possible early discharge for outpatient management.
The recent clinical introduction of high-sensitivity cardiac troponin T (hs-cTnT) testing using the European Society of Cardiology (ESC) 0-hour/1-hour (0h/1h) algorithm means that suspected AMI cases in the emergency department can now be diagnosed in as fast as 1 hour, which translates into improved clinical outcomes and reduced costs for healthcare systems.
Successful implementation of the algorithm in the hospital setting requires the concerted efforts of multi-disciplinary teams including clinical lab professionals, emergency department (ED) physicians, cardiologists and nurses. This article provides a brief introduction to the 0h/1h algorithm, the role of the lab in making it possible, and its benefits for patients, clinicians and providers.
The 0h/1h Algorithm Principle
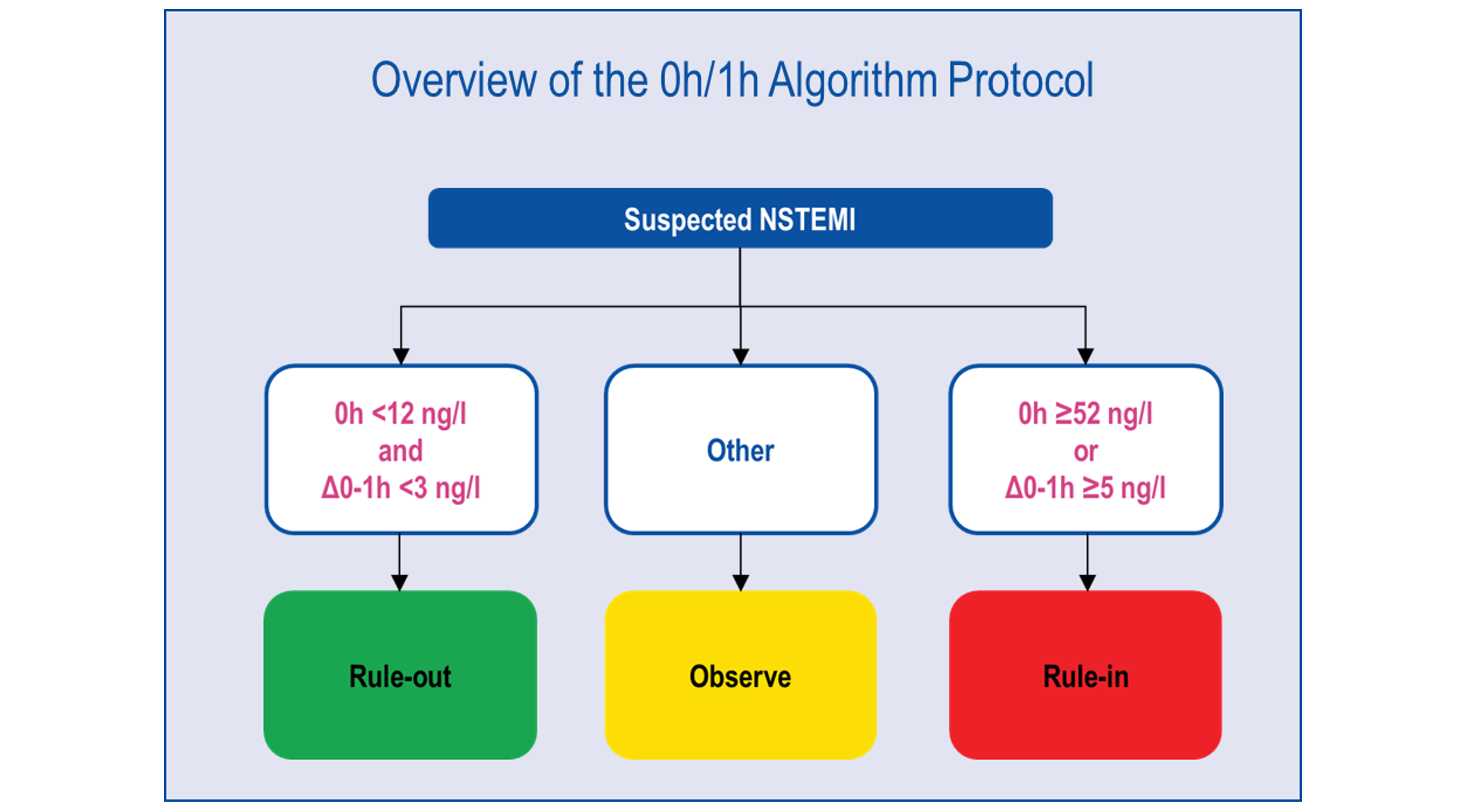
The 0h/1h algorithm is a widely validated protocol recommended by the ESC to provide rapid disposition of patients into ‘rule-in’ or ‘rule-out’ AMI in 1 hour when hs-cTnT is available.
A low baseline troponin concentration of less than 12ng/L at 0h and concentration change of <3ng/L within 1 hour qualifies for ‘rule-out’; a high baseline troponin that is greater than or equal to 52ng/L at 0h and concentration change of ≥5ng/L within 1 hour qualifies for ‘rule-in’. Patients who do not fulfil either criteria are placed into the ‘observe’ zone (see Figure 1 below).
In a recent series of interviews with Roche Diagnostics Asia Pacific, cardiologists and ED physicians from King Chulalongkorn Memorial Hospital in Thailand and Juntendo University Nerima Hospital in Japan—two hospitals in the Asia Pacific region that have successfully adopted the 0h/1h algorithm for AMI diagnosis—shared their experience with the implementation and the positive impact on patient care and outcomes.
The Critical Role of Clinical Labs
In patients with suspected AMI, labs must ensure rapid turnaround time (TAT) of the hs-cTnT to enable the accurate interpretation of the change in cardiac troponin over 1 hour.
“Nowadays, lab tests are not just simply about quality and accuracy,” said Dr Chintana Chirathaworn, Associate Professor at the Department of Microbiology at Chulalongkorn University in Thailand. “Today, we need to focus more on speed and fast turnaround time so that clinicians can diagnose and assess patients quickly.”
Some of the key factors that are driving lab efficiency to make the 0h/1h algorithm possible include pre-analytical units for rapid sample processing, automated detection systems that produce test results within minutes, information systems that send results directly to clinicians, and auto-validation systems for quality control and delta checks.
Active participation of the lab members in discussions with the involved physicians is also important to ensure accuracy of the test results and adherence to the required protocols. “We need to know what kind of tests the doctors want, and how they want it to properly diagnose the patients,” Dr Chirathaworn added.
Steps to Ensure Rapid TAT for the 0h/1h Algorithm
“When we first used the 1-hour algorithm, we sometimes could not get the results back within 1 hour,” said Dr Wacin Buddhari, who directs the Cardiac Catheterisation Laboratory at King Chulalongkorn Memorial Hospital. “Therefore, we had to adjust a few things to be able to receive test results within 1 hour, from the process of sending the blood sample, the test procedure, and the reporting of results.”
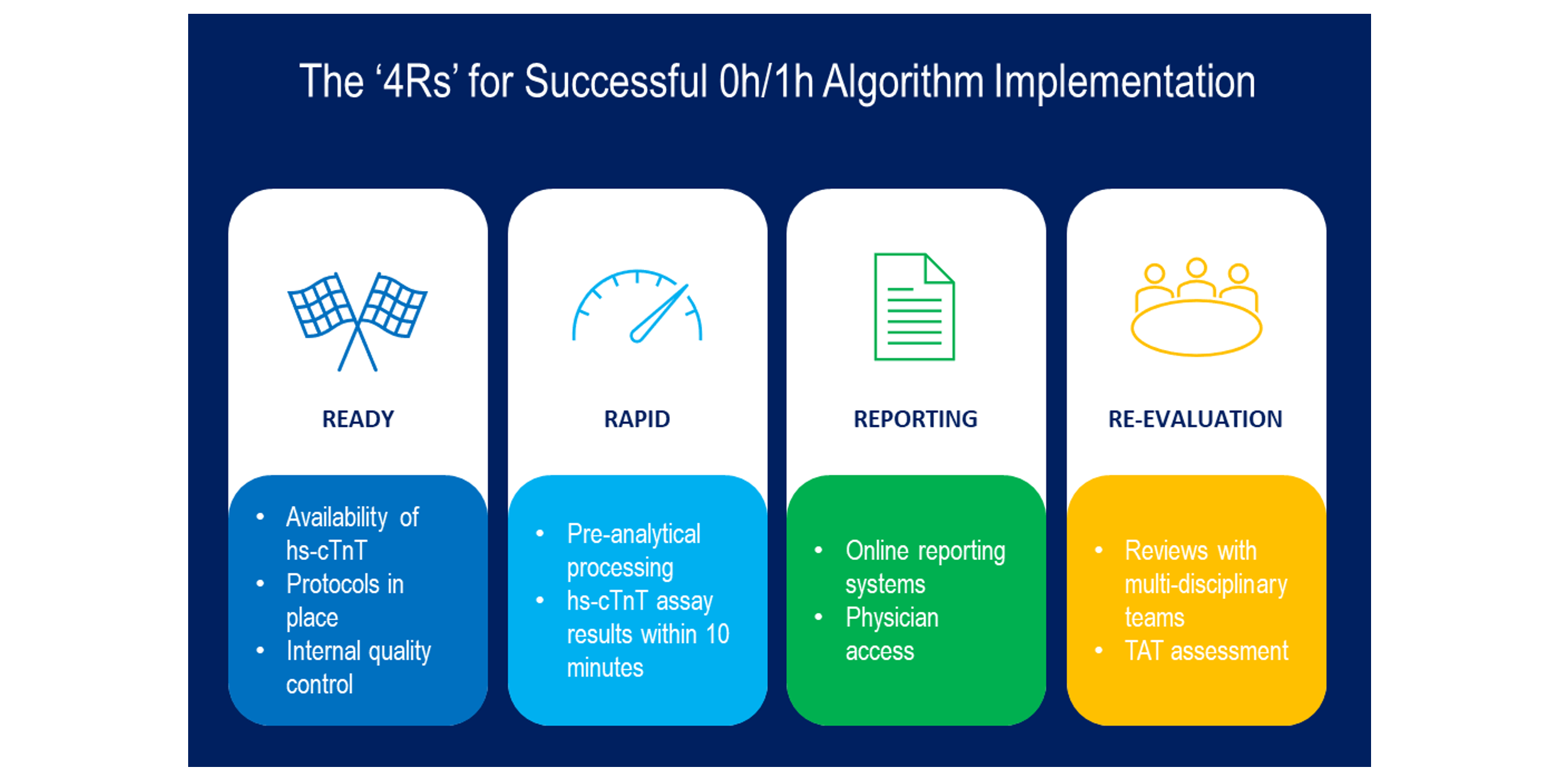
Dr Chirathaworn described ‘4Rs’ that the clinical lab at King Chulalongkorn Memorial Hospital considers important to ensure fast TAT and successful implementation of the 0h/1h algorithm (see Figure 2 below).
For patients, the 0h/1h algorithm can improve safety and clinical outcomes. Rapid exclusion of AMI can significantly reduce the waiting time and anxiety of patients and their family members in the ED. The high negative predictive value of the 0h/1h algorithm also ensures more precise diagnosis, which increases confidence in clinical assessments, particularly ‘rule-out’ cases where physicians can safely send patients back home.
“In caring for patients with acute chest pain from myocardial infarction, we often hear the term ‘time is muscle’, indicating that the earlier we can detect and initiate treatment, the more myocardium can be saved,” said Dr Krongwong Musikatavorn, Assistant Professor and Head of Emergency Medicine Department at King Chulalongkorn Memorial Hospital.
Benefits for Clinicians and Providers
Clinicians also benefit from implementation of the 0h/1h algorithm. Since the algorithm provides an objective and absolute index, it enables non-cardiologists and young or night shift doctors to make critical decisions when assistance may be unavailable. At Juntendo University Nerima Hospital, ED physicians are also sometimes hesitant to seek consultation from cardiologists without a solid basis for assessment.
For providers, fast and accurate triage of patients can reduce overcrowding in the ED and non-essential hospitalisation, freeing up resources including bed spaces and physicians for other critical patients. Reduced emergency cardiac catheterisation exams may also vacate bed spaces and spare patients from the risk of associated complications.
Rapid TAT and reliable processes in the clinical lab make all these benefits possible. By supporting implementation of the 0h/1h algorithm, hospital labs can play a central role in improving patient care while simultaneously demonstrating clear value to all their key stakeholders.
Want to learn more about the 0h/1h algorithm and how it is being implemented in the Asia Pacific region? Check out Cardio Thinklab, a scientific educational portal on cardiovascular disease management.





