
 Article
Article
Any paediatrician will tell you that kids are not just “little adults”—the fact that they are growing and developing means their body systems process things differently than adult bodies. It makes sense that this difference between child and adult metabolism impacts laboratory values.
Many common lab tests have different ideal cut–offs for normal values between children and adults, including complete blood count, coagulation, blood chemistry and procalcitonin. In many cases, there are several age groups with differing cut–off values, so paying attention to patient age can be critical in determining whether results are abnormal.
Blood clotting
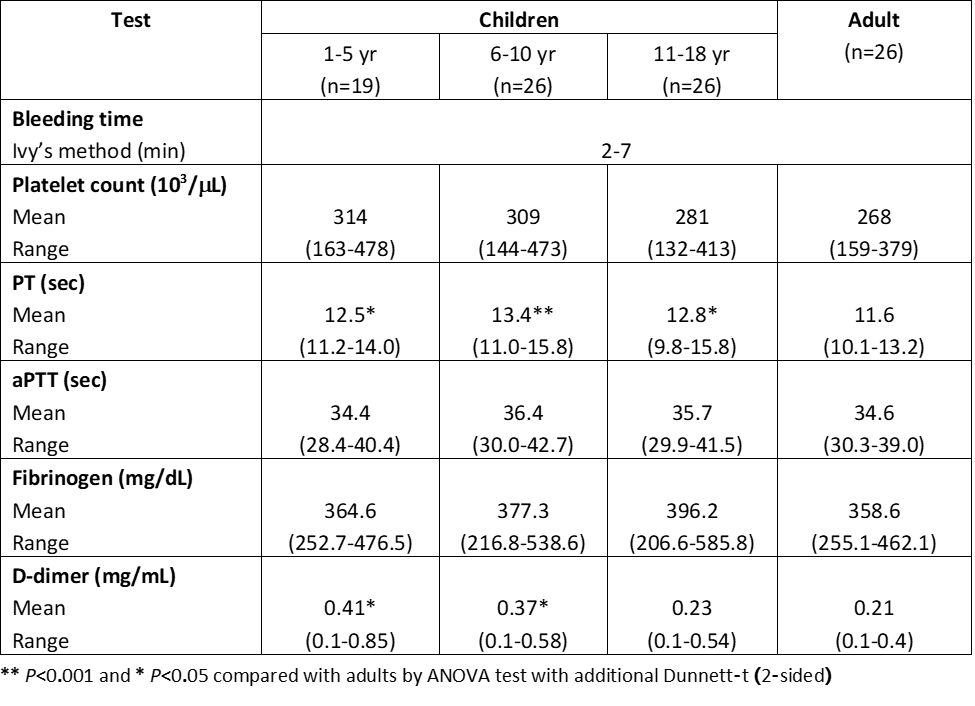
Some resources divide reference range values into six or more age groups for normal results in children. A prime example of the differing ranges for normal laboratory values in children can be found in coagulation tests, such as prothrombin time (PT) and activated partial thromboplastin time (aPTT). If adult reference ranges were used for coagulation tests such as PT and aPTT, as many as 30% of kids aged 1 – 10 would be labelled as abnormal, resulting in unnecessary follow–up tests or diagnostics. For these tests in particular, normal values don’t only depend on regular post-partum age, but also gestational age for infants born prematurely [1].
Anticoagulant markers have similar differences by age group. For example, the natural anticoagulant protein C antigen activity has a mean value of 63.0% for children under the age of 1 year, but a mean of up to 90.7% for adults [2]. Values do not always change in a linear fashion either—many times, values and normal ranges go up or down based on life stages such as infancy or puberty. To correctly interpret thrombotic markers in anyone, knowing the patient’s age is essential.
Blood chemistry
Blood chemistry tests inform follow-up examinations and additional testing for many diseases. Since normal values can differ considerably for kidney function, liver function, iron profiles and other tests based on a child’s age, it is crucial to use accurate cut-offs based on patient age.
Some common tests, such as those for inorganic phosphorus and potassium, even vary in normal ranges from day to day for newborns. For example, a baby with a potassium level of 3.2 mmol/L would be normal in the first week of life, but below the lower limit by the second week of life.
In addition, the common distinction between male and female reference ranges in adults sometimes also applies to children. For example, an alanine aminotransferase (ALT) value of 8U/L for a 10-day-old baby is normal for females, but below the reference age for male newborns.
Make age-based reference values easier for your lab
If it’s not already standard practice for your lab to check patients’ ages before reporting results, here are a few tips:
- Consult your country’s laboratory quality organisation or professional practice group to obtain the latest paediatric reference ranges for all tests your laboratory performs.
- For updates on paediatric reference range initiatives [2] around the globe, review resources created by the Task Force on Paediatric Laboratory Medicine—part of the International Federation of Clinical Chemistry and Laboratory Medicine.
- Post age-based reference range tables for common tests in plain view. For example, keep them on the wall near laboratory equipment or your reporting station. Open-access publications offer thorough and recent tables for normal paediatric ranges for dozens of common tests [3].
- If you have an automated result reporting system, make sure that the programme reports findings based on age-based reference ranges.
- Train your staff on the difference between paediatric and adult reference ranges. By teaching them about the differences—and showing them the cut-off charts—you can help keep the topic top of mind.
- Add an age check to your lab’s quality assurance protocol or reporting checklist (such as this checklist by the World Health Organisation [4]) This will ensure that all results are reviewed for patient age. If the patient is a child, results should also be checked against paediatric reference ranges before calling physicians or mailing results.
By implementing these simple strategies for paediatric testing, you can save patients and physicians unnecessary expense, stress and time. In addition, you can feel confident that you are following the latest standards for paediatric laboratory reporting—and saving your laboratory resources for follow-up tests that are truly needed.
[1] Lanzkowsky’s Manual of Pediatric Hematology and Oncology 6th edition
[2] IFCC Paediatric Reference Range Initiatives. https://www.ifcc.org/ifcc-emerging-technologies-division/etd-committees/c-etplm/paediatric-reference-range-initiatives/
[3] Paediatric normal laboratory values, Appendix B.
[4] World Health Organisation Laboratory Quality Stepwise Implementation tool checklist
This article was based on a presentation: Value of Laboratory for Pediatrics at Roche Scientific Days 2018: Empowering Lab Leadership to the Next Level in Dusit Thani Hua Hin, Thailand.





